A fter an episode of anxiety associated with performing, I feel strange—like I’m empty and numb. It feels like I am watching everyone else, but at a distance. It’s not an ‘out-of-body experience’ or anything like that. Not light-headed or dizzy. But I do feel short of breath—my breathing is fast, and my heart-rate is still fast—even though the performance is over and the reason for the anxiety is over. It’s really weird. I just feel like there’s a ‘distance’—like the other people are real and I am somehow not real. It makes me feel so alone. It goes on for hours. Usually I have to go to sleep, and when I wake up the next day I feel completely normal. Is this some ‘after-effect’ of anxiety or what? Is this what it feels like after a seizure or something?”Since my previous posts on the stage-fright topic, I’ve received several comments/questions similar to the one above.
— Anonymous.
The neurologic state associated with an episode of stage fright is not an epileptic one. But the sensations afterward can feel almost ‘inter-ictal’, with some qualities similar to what people who’ve experienced a seizure feel. And Panic Disorder and PTSD share many clinical features—such as ‘anticipatory anxiety’ and depression and ‘intrusive imagery’—imagined potential scenarios that bug you. Functional MRI and other studies of regional cerebral blood flow are beginning to show similarities, too. So the after-effects of a solo concert—feeling like you may have PTSD—aren’t really that surprising, neurologically or physiologically speaking.
Some of you who’ve sent me comments have wondered whether there are objective ways to measure the severity of the anxiety you’ve experienced. Clinically, there are a variety of scores that are used, but most of them are lengthy questionnaires, and very few of them have been designed to be self-administered. The one by Snaith and colleagues is short, intended for self-admin, and it does address ‘panic attacks’. This is different from stage-fright per se, but it nonetheless might be a helpful and relevant gauge, for those of you who’ve asked about this. Here’s a spreadsheet I’ve prepared. You can download it by clicking on this screenshot.

Panic Disorder (in the DSM-IV diagnostic nomenclature) is characterized by recurrent panic attacks—that is, periods of intense anxiety—in which 4 (or more) of the following symptoms develop abruptly and reach a peak within 10 minutes:
- palpitations, pounding heart, or accelerated heart rate;
- sweating;
- trembling or shaking;
- sensations of shortness of breath;
- feeling of choking or dry mouth and dry throat;
- chest pain or discomfort;
- nausea or abdominal distress;
- feeling dizzy, unsteady, lightheaded, or faint;
- de-realization (feelings of unreality) or de-personalization (being detached from oneself);
- fear of losing control;
- fear of collapsing or dying;
- paresthesias (numbness or tingling sensations);
- chills or hot flashes.
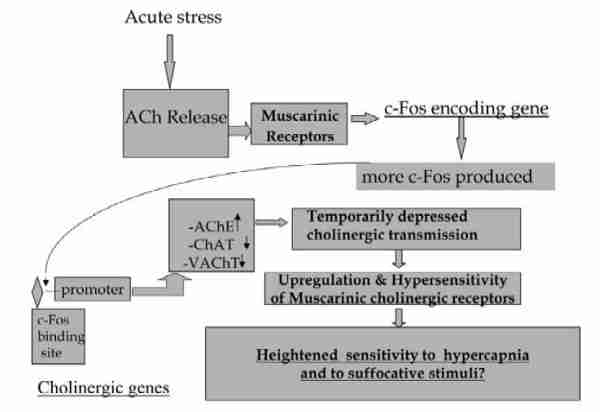
It turns out that central (brain) muscarinic cholinergic receptors are involved in our physiologic reactions to these stimuli (see the Battaglia chapter in Silman’s book for a short summary), including slight increases in CO2 in the bloodstream. The slight elevation of CO2 (hypercapnia) is what triggers the faster breathing and the racing heartbeat. And the acute stress causes an increase in the release of acetylcholine in the hippocampus in the brain (see Kaufer paper) that has a several-hours duration. Concomitantly, about 70% of people subject to panic attacks have increased sensitivity to lactate in the bloodstream, compared to healthy normals (Rosenbaum, p. 63). And that triggers faster breathing at lower blood lactic acid concentrations—at far lower levels of lactate than would cause hyperventilation in ‘normal’ unstressed people.
Also, recent research has shown that in panic attacks there’s an up-regulation of gene expression of cholinergic muscarinic receptors, cFOS, and other gene products. That up-regulation also lasts for hours—and is related to the increased sensitivity to CO2 and lactate.
In fact, since I’m not personally affected by panic attacks or stage-fright and since I don’t have any work-related reason to intensively follow the medical literature on the subject, I hadn’t previously seen the articles on anticholinergic drugs and panic attacks. But there’s actually quite a lot of new evidence for cholinergic causation of panic—accumulating evidence over the past 5 to 8 years or so. It’s not the sort of thing that your average GP would know about.
Curiously, inhibitors of the enzyme acetylcholinesterase (AChE) [for example, Alzheimer’s drugs, like donepezil (Aricept™), rivastigmine (Exelon™) and galantamine (Reminyl™); also neostigmine (Prostigmin™), pyridostigmine (Mestinon™) and other various cholinergic drugs used to treat myasthenia gravis] may induce sensations and cognitive changes that are reminiscent of post-traumatic stress disorder (PTSD), including de-personalization or feeling ‘distanced’ or unreal—very much like the symptoms described by the conservatory-student commenter above.
In other words, you can increase the number of acetylcholine receptors, or you can increase the sensitivity or binding affinity of the existing receptors, or you can increase the concentration of acetylcholine molecules available to bind to those receptors (by inhibiting AChE, the enzyme that metabolizes acetylcholine)—any of these changes can produce the same distinctive cognitive symptoms.
And, logically, you might think that doing the opposite—for example, using a drug that inhibits the binding of acetylcholine to the receptors, or a drug that enhances the activity of the AChE enzyme, or a drug that down-regulates the gene expression of the receptor or that post-transcriptionally changes the sensitivity of the receptors expressed—might offer some relief or prevent such symptoms. Yes, it’s been tried. Transdermal scopolamine and other strong anticholinergics don’t necessarily help panic attacks, though. But Battaglia’s work in Italy suggests that low doses of Akineton™ (biperiden, a weak anticholinergic drug) can help [see 2001 paper published in Arch Gen Psych ]. Anecdotal reports of the off-label use of biperiden for stage-fright also exist, although they’re not nearly as common as ones reporting the use of beta-blockers.
Of the various options, the biperiden should be relatively less likely to cause performance problems, compared to the others—compared to SSRIs, say. But, hours after the performance, brain cholinergic activity decreases below baseline. And then biperiden’s lingering activity (it has a 18 to 24-hour half-life) might be annoying—the day after your performance.
A noradrenergic (catecholamine) mechanism of panic has been substantially repudiated in the past 15 years. Clonidine and other alpha-blockers are ineffective—that’s part of the evidence. And plasma and urine MHPG levels are not usually abnormal in the way one would expect if noradrenergic overactivity were the cause. And SSRIs are effective in panic attacks, which one would not expect if noradrenergic overactivity were the cause. In other words, the catecholamines in panic attacks seem to be the ‘effect’, not the ‘cause’. The beta-blockers mentioned in previous posts essentially address these ‘effects’, not the ‘causes’.
Serotonergic abnormalities are at least partly implicated—especially the 5-HT(1A) receptor—and this is the basis for the use of buspirone (Buspar™) or risperidone (Risperdal™) in panic disorder. GABAA / Benzodiazepine receptors (see Goddard, Gorman & Charney in Rosenbaum, pp. 57-92) have also been implicated—and that fact gives rise to another avenue of treatment/prevention possibilities.
The information on this page is not intended as medical advice and is not meant to be a substitute for individual medical judgment by a physician or other medical healthcare professional. The aim is to provide information and help in suggesting considerations for preventive care. The medications listed below should be used only after a medical examination and under the supervision of a doctor. Always consult a licensed healthcare provider for individualized advice on your health decisions.
- Medications that have been used in Panic Disorder
- Anticonvulsants [levetiracetam (Keppra™, 500 mg bid)]
- Serotoninergics [risperidone (Risperdal™, 4 mg qd, 5-HT(1A) and 5-HT(2) antagonist), buspirone (Buspar™, 10 mg bid, partial 5-HT(1A) agonist)]
- SSRIs [paroxetine (Paxil™, 20 mg qd), sertraline (Zoloft™, 50 mg qd), fluoxetine (Prozac™, 20 mg qd), fluvoxamine (100 mg qd), citalopram (Celexa™, 20 mg qd), escitalopram (Lexapro™, 10 mg qd)]
- Benzodiazepines [alprazolam (Xanax™, 1 to 4 mg qd), lorazepam (Ativan™, 2 mg qd), clonazepam (Klonopin™, 1 mg qd). ]
- Anticholinergics [biperiden (Akineton™, 2 mg qd), possibly trihexyphenidyl (Artane™, 1 mg qd)]
Hope this helps. Let me know how things go, if you decide to pursue any of these things.
Incidentally, it’s unknown how occasional stressful events [like recitals] might mediate long-term neuronal plasticity in the brain. And it’s unknown whether repeated high-anxiety episodes of the sort experienced by some performing chamber musicians could lead to PTSD or, if they can in some cases lead to PTSD, how frequent or severe the episodes have to be to have a high probability of doing so. We won’t worry about it, since it seems not to have been examined in clinical trials or other studies. But the absence of evidence is not evidence of absence, and all that…
- National Anxiety Foundation
- Anxiety Disorders Association of America
- Anxiety Network
- National Institute of Mental Health (NIH) page on panic disorder
- RESPeRATE biofeedback trainer (InterCure Ltd.; Amazon distributor)
- RESPeRATE biofeedback trainer (InterCure Ltd., Israel; MindFitness distributor)
- RESPeRATE FDA K020399 510(k) clearance summary [1MB pdf]
- Bassett L. From Panic to Power: Proven Techniques to Calm Your Anxieties, Conquer Your Fears, and Put You in Control of Your Life. Collins, 1997.
- Battaglia M, Ogliari A, Villa F, Ferini-Strambi L, Maffei C. Human panic disorder and the cholinergic system, in Silman I et al, eds., Cholinergic Mechanisms. Informa, 2004, Pp. 463-6.
- Battaglia M. Beyond the usual suspects: a cholinergic route for panic attacks. Mol Psych 2002; 7:239-46 [0.2MB pdf]
- Battaglia M, Bertella S, Ogliari A, Bellodi L, Smeraldi E. Arch Gen Psych 2001; 58: 114-9. [0.1MB pdf]
- Bemis J. Barrada A. Embracing the Fear: Learning To Manage Anxiety & Panic Attacks. Hazelton, 1994.
- Carbonell D. Panic Attacks Workbook: A Guided Program for Beating the Panic Trick. Ulysses, 2004.
- Emilien G, Durlach C, Leopola U, Dinan T. Anxiety Disorders: Pathophysiology and Pharmacological Treatment. Birkhauser, 2002.
- Fehm L, Schmidt K. Performance anxiety in gifted adolescent musicians. J Anxiety Disord 2006; 20: 98-109.
- Heninger G. Catecholamines and the pathogenesis of panic disorder. Arch Gen Psych 1998; 55:522-3.
- Kaufer D, Friedman A, Seidman S, Soreq H. Acute stress facilitates long-lasting changes in cholinergic gene expression. Nature 1998; 393:373-7.
- Kenny D, Osborn M. Music performance anxiety: New insights from young musicians. Adv Cog Psychol 2006; 2:103-12. [1MB pdf]
- McNally R. Panic Disorder: A Critical Analysis. Guilford, 1994.
- Pargman D. Managing Performance Stress: Models and Methods. Routledge, 2006.
- Rosenbaum J, ed. Panic Disorder & Its Treatment. Informa, 1998.
- Snaith R, Baugh S, et al. The Clinical Anxiety Scale (CAS): An instrument derived from the Hamilton Anxiety Scale. Brit J Psychiat. 1982; 141: 518-23.
- Wilson R. Don't Panic: Taking Control of Anxiety Attacks. Harper Collins, 1987.
- DSM. High Anxiety: Prazosin and Other Alternatives. CMT blog, 12-NOV-2007.
- DSM. Managing Stage Fright & Performance Anxiety in Classical Musicians. CMT blog, 17-MAY-2007.
No comments:
Post a Comment