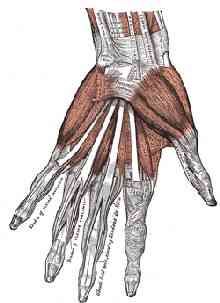
S till having tenderness and weakness in my left hand when I’m playing lute. What exercises should I try? Are there any exercises that I should stay away from—ones that could do more harm than good? Is there any exercise equipment that can make the muscles in my hand stronger, but not make the control coarser or less precise? Wrapping the wrist—would that help maybe? What about wrapping the fingers—especially the middle finger and the ring finger—how about that?”The lumbricals are four small muscles in each hand that interconnect the deep flexor muscles to the extensor muscles of the fingers. The lumbricals are the only muscles in the human body that have no direct bony attachments. They attach at both ends to tendons of these other muscles. The lumbricals are extensors of the proximal interphalangeal (PIP) and distal interphalangeal (DIP) joints. In addition, the lumbricals play a part in side-to-side and rotation movements of the fingers. They’re metacarpal phalangeal (MCP) joint flexors as well, but they’re relatively weak as flexors. They get fatigued easily in their flexor and abductor-adductor and rotator roles.
— Anonymous.
As each finger moves through its range of motion, each tendon slides a certain distance (An, 1983; Storace and Wolf, 1982). Excursion takes place simultaneously in the flexor and extensor tendons during joint motion: the tendons of the agonist muscles displace in one direction, while the tendons of the antagonist muscles displace in the opposite direction. Knowing what the tendon excursions are has applications for rehabilitation or enhancement of the hand (Brand and Hollister, 1999; Chao, 1989). Most of the time, your exercises should involve motions that cover most of the normal excursion that the tendon (and joint) moves through.
| Muscle | Tendon Excursion (mm) |
| Interossei | 30 |
| Extensor pollicis brevis | 30 |
| Abductor pollicis longus | 30 |
| Lumbricals | 40 |
| Thenar muscles | 40 |
| Finger extensors | 50-60 |
| Finger flexors | 60-70 |
Coordination is usually tested by counting the number of repetitions of a particular movement—such as rapid repeated tapping—that you can do in 30 seconds. Reduced ability to perform rapid, repetitive movements is often seen for movements that involve muscles like the lumbricals and interossei muscles. Try tapping with each finger of each hand and record your results. The repetitive movement is fatiguing, and you may find you need to concentrate more to perform the test on one side compared with your other side. Lack of precision and lack of smooth movement often are observed, with noticeable differences between fingers and between the two hands. Doing this testing is, admittedly, a bit tedious. But you’ll have a clearer and objective idea of your situation if you do these timed counts.
Subtle issues of coordination and endurance may be more of a problem in lute players than many other musicians—because of the geometry of the instrument. Correcting muscle imbalance requires stretching tight muscles—soft tissue massage. Often a particular area is painful, and ‘trigger points’ are found in the corresponding muscles. Common trigger point sites often include the dorsal first, second, and fourth interossei, the middle finger common extensor, the extensor indicis, the flexor carpi radialis, and flexor carpi ulnaris muscle bellies. You ‘find’ the trigger points by palpating with your right hand’s fingers while you make the left hand do the motions/excursions that are problematic.
Correcting muscle imbalance also requires strengthening the weaker muscles—extensor carpi ulnaris, common wrist extensors, and intrinsic muscles of the hand including the lumbricals. Specific lumbrical muscles surrounding a painful finger are often weak. If you have a lax, hyperextended thumb, it may have a weak extensor pollicis brevis. Often the thumb opponens and flexor pollicis brevis muscles are weak but the thumb adductor muscle is pretty strong. Treatment for hyperlaxity includes temporary supports and strengthening exercises.
Temporary supports to maintain a joint in a neutral position can be helpful. You can gradually wean yourself from them as your symptoms subside and the finger strength improves. Supports may include neoprene wraps or Lycra finger sleeves. These provide joint stability for hypermobile thumb, finger, or wrist joints. The tough thing is to find a support that’s not too bulky or stiff. The reinforced Lycra sleeves that are used for volleyball and other sports aren’t flexible enough. Some Lycra sleeves of the types that are sold in pharmacies are too flexible and don’t offer enough support. Other finger sleeves of the types sold by fly-fishing retailers have a millimeter or two of neoprene or other materials that are too bulky.



The DigiSleeve product is, for me, a reasonable compromise between support and flexibility. It comes as a length of Lycra tube that you cut with a scissors to the exact length that’s right for the dimension of your finger and the amount of the phalanges that you want to cover or support. It’s fairly inexpensive—you just discard the tube segments after several episodes of use and cut yourself new ones. I made a ‘template’ measuring guide on a postcard where I marked off the lengths that I need for the fingers I use the DigiSleeves on, and I keep this template card on my desk next to the box where I keep the DigiSleeve materal. When I need a new sleeve, I just lay the DigiSleeve material on the appropriate template “finger” on the card and cut with a scissors to the right length for that finger. Quick, easy, no re-measuring or guessing, and no wasted material.
In general, it takes some months for joint stability and lumbrical muscle strength to improve significantly, so you’ll need some patience with the temporary splints or wraps and a modified playing schedule. ‘Stability strengthening’ exercises encourage co-contraction of the muscles surrounding a joint. Improved stability strength helps to compensate for a hyperlax joint. Stability strength training can include isometric and proprioception exercises on your instrument and on exercise equipment like the kinds shown here. For exercises away from the instrument, you can do muscle contractions with a support (such as Lycra finger sleeves) on.


In later phases, your hand exercises can include strength training motions that are are concentric and eccentric (with respect to the center of rotation around the affected joint). The DocZac device works pretty well for this. ‘Proprioception’ exercises can include tapping and weightbearing—mostly in a mid-range, neutral joint position. Finger push-ups for hyperlax finger joints, for example—can be performed anytime, against a table or other convenient surface.


Warrington emphasizes that even the most conscientiously developed exercise program cannot reproduce exactly the action required from the various joints and muscles to play your instrument. And, yes, performing exercises that reproduce some of the actions and that aim to strengthen certain muscles, like the lumbricals, or aim to reduce the laxity of certain joints can be carried too far—excessive exercise can lead to further imbalance or overuse injuries or inflammation, can lead to different problems than the ones the exercises were designed to solve. You’ll be best able to judge your progress—and keep an eye out for problems that may develop—if you keep a log and record your daily hand exercise routine and other relevant details.

There are fancy, expensive equipments that neurologists use to measure these things. But there are also some freeware/shareware programs that you can use on your computer to do pretty much the same measurements. One of these is Stamina 2.5 (Windows XP / Vista). You can create your own ASCII script files, tailoring the sequence of key-depressions to just those motions that you want to work on or measure, in each of the fingers you are having problems with. From the Stamina 2.5 pull-down Mode menu, choose Other Modes. Select the External File cascading menu choice and navigate to the .txt file you want. Here is one I created for the left ring-finger, and here is one I created for the right ring-finger. Download them and save them to a directory on your PC as you prefer, or to the c:\Program Files\Stamina\Data\ subdirectory where the script files for Stamina 2.5 reside. You can use these as-is, or, more likely, just examine them and see how you may want to set up your own custom script files. Besides revealing the characters-per-minute (cpm) count, which you can record in your daily log, Stamina 2.5 shows the graphical time-trend of how your fingers fatigue with prolonged action. As your stability-strengthening exercises proceed, you may notice that the rate at which your lumbricals-propelled fingers fatigue gets better as the muscles get stronger. And if you experience an injury, the graph is a sensitive indicator of the injury and its severity. The lower cadence achieved by the ring finger may be due more to a lack of independence at the level of voluntary neuromuscular control, than to any innate mechanical interaction with (‘enslavement’ to) the other fingers. Tapping cadence of each finger is lower for the double-finger mode than for the single-finger mode.
You can know for certain when your fingers are being moved by the lumbricals—just make your fingers do a harp-plucking motion. Generally, the lumbricals, flexors, and extensors will all be involved at once, in a way not under your conscious control. Change the finger movement—change the relative amount of straightening and forward motion—and feel your left forearm with your right hand. If the flexor and/or extensor muscles in your arm are contracting, you distinguish it easily because those muscles grow thicker and slide under the skin. When you’re moving your finger forward in such a way that you can’t feel much muscular action in the forearm, then the lumbrical muscle is doing almost all the work. Here are four basic rules for achieving accurate control and endurance:
- Do not make unnecessary movements or muscle contractions.
- Do the necessary movements as smoothly as possible.
- Use the strongest muscles that can do the job.
- Exercise to strengthen the muscles that have the potential to do the job.
- DSM. Lutes and Lumbricals. CMT blog, 29-APR-2007.
- Stamina 2.5 (Windows freeware; 1.3MB download)
- External character file to measure left 4th digit tapping speed in extension and flexion, for Stamina 2.5 software [4KB txt file]
- External character file to measure right 4th digit tapping speed in extension and flexion, for Stamina 2.5 software [4KB txt file]
- Chartered Society of Physiotherapy, U.K.
- Center for International Rehabilitation Research Information and Exchange (CIRRIE)
- Leijnse J. Why the Lumbrical muscle should not be bigger—a force model of the lumbrical in the unloaded human finger. J Biomechanics 1997; 30: 1107-14. [1MB pdf]
- DigiSleeve (cut to desired length with scissors)
- Alpine Innovations Stripee fly-fishing finger guards
- Futuro support glove
- Gripmaster hand exerciser, extra-light tension
- DocZac Handmaster-Plus exerciser
- Expand-Your-Hand bands
- An K-N, Chao E, Cooney W, Linscheid R. Forces in the normal and abnormal hand. J Orthop Res 1985; 3: 202-11.
- Aoki T, Furuya S, Kinoshita H. Finger-tapping ability in male and female pianists and nonmusician controls. Motor Control. 2005;9:23-39.
- Aoki T, Francis P, Kinoshita H. Differences in the abilities of individual fingers during the performance of fast, repetitive tapping movements. Exp Brain Res. 2003;152:270-80.
- Brand P, Hollister A. Clinical Mechanics of the Hand. 3e. Mosby, 1999.
- Brookfield J. Grip Master's Manual. IronMind, 2002.
- Brookfield J. Mastery of Hand Strength. IronMind, 1995.
- Chao E, An K-N, Cooney W, Linsheid R. Biomechanics of the Hand: A Basic Research Study. World Scientific, 1989.
- Christianson M, Leathem J. Development and Standardisation of the Computerised Finger Tapping Test: Comparison with other finger tapping instruments. New Zealand J. Psych. 2004; 33:.
- Green J, Champagne P, Tubiana R. Prevention, in Tubiana R, Amadio C, eds. Medical Problems of the Instrumentalist Musician. Martin Dunitz, 2000, pp. 540-8.
- Horvath J. Playing (Less) Hurt. Horvath, 2006.
- Jobbágy A, Harcos P, Karoly R, Fazekas G. Analysis of finger-tapping movement. J Neurosci Methods. 2005;141:29-39.
- Paull B, Harrison C. The Athletic Musician: A Guide to Playing Without Pain. Scarecrow, 1997.
- Sataloff R, Brandfonbrener A, Lederman R. Performing Arts Medicine. 2e. Singular, 1998.
- Storace A, Wolf B. Kinematic analysis of the role of the finger tendons. J Biomech 1982; 15:391-3.
- Warrington J. Hand therapy for the musician: Instrument-focused rehabilitation. Hand Clin 2003; 19:287-301.
- Warrington J. Upper-extremity Problems in Musicians Related to Age. MPPA 2002; 131-4. [500KB pdf]
- Devonshire Hand Clinic, 30 Devonshire Street, London, W1G 6PU, Tel: +44 020 7486 7131, Email: j.warrington@tesco.net
- Winspur I, Wynn Parry C, eds. The Musician's Hand. Taylor & Francis, 2005.

No comments:
Post a Comment